



SHOCKING WHIPLASH INJURY STATISTICS:
- Journal of the American Academy of Orthopedic Surgeons, 2007
- seemingly unrelated health problems. Journal of Clinical Epidemiology, 2001
- not been shown to improve the pain nor the psychological profiles of people suffering from the effects of their automobile accident. Pain, 1997
- Accident Analysis and Prevention, 2002
- Spine, 2000
- Injury, 2005
- Pain, 1994
"" Orthopedist and one of the world's foremost experts on whiplash, Dr. Dan Murphy. There are 3,000,000 new cases of whiplash in the US every year.
WHAT IS WHIPLASH?
When people think of “whiplash” they tend to think of motor vehicle accidents (MVA’s). Although MVA are probably the single most common cause of the symptoms most frequently associated with and experienced by those suffering with Whiplash Associated Disorders (neck pain, upper back pain, shoulder pain, fuzzy thinking, numbness, tingling and / or weakness of the hands, dizziness, etc), whiplash can occur in many other different ways. There are certain symptoms that we see over and over and over in our clinic (neck pain and headaches, for instance). Whiplash can seemingly cause many other symptoms as well. Some of the most common causes of WAD that we see in our office include sports injuries, work injuries, horse accidents (falls), physically fighting, and almost anything else that has the capacity to “snap” your head suddenly and violently.
Although the most common problems associated with Whiplash Associated Disorders are related to the neck (neck pain, numb hands, headaches), scientific research shows that Acceleration / Deceleration injuries routinely cause all sorts of other injuries as well. We commonly see people whose low back pain started with an MVA. We even see people whose Fibromyalgia was brought on by the emotional and physical stress of an Motor Vehicle Accident.
Even though there are literally scores of scientific studies concluding that Whiplash Associated Disorders are difficult (often to the point of being impossible) to image on x-rays, CT's, or MRI’s, these are still the chief methods the medical community is using to determine whether or not you were injured, and just how serious this injury might be. The problem is, if the vast majority of soft-tissue injuries (injuries to Ligaments, Tendons, Muscles, Fascia, etc) do not image well with advanced imaging techniques, and imaging is the medical community’s chief method of diagnosis; unless you have a herniated disc, you will invariably be treated like nothing is really wrong with you. Stop and think for a moment about how problematic that fascia, arguably the single most pain-sensitive tissue in your entire body, will not show up on any tests, including an MRI.
When you are taken the the ER, you will have some tests run and the doctor will look at you and say, “Well it is a good thing Mrs. Smith, nothing is broken. Here are a couple of prescriptions for any pain and/or inflammation you may have from now until you see your family doctor tomorrow. In the mean time, wear this collar and use a warm pack when needed." Is this good advice? Sure it is, if you own a medical clinic. Followthis advice and you are certain to become a lifetime Arthritic. The truth is, when it comes to the evaluation and treatment of injuries to fascia and other elastic, collagen-based connective tissues, all of our hi-tech equipment with its bells and whistles is simply not helping diagnose or help most injured people. Our DIGITAL MOTION X RAY (DMX) has helped many patients in your same shoes.We encourage you to visit our website dmxofwisconsin for further information.
Many of you reading this and suffering with Whiplash Associated Disorders do not have a history of MVAs. It is important that you understand that a MVA is certainly not the only way that people end up with WAD. It is absolutely critical that anyone who thinks that they might be suffering the effects of a whiplash-like injury, learn a little bit about COLLAGEN-BASED, ELASTIC CONNECTIVE TISSUES. Knowledge is power. You will either educate yourself or be taken advantage of and used as a guinea pig for the latest drugs and procedures!
BRAIN-BASED THERAPY:
Your short drive to work was no different than any other day, until you began slowing down for the school bus stopping in front of you. Just as you're coming to a complete stop, CRASH; your world explodes as someone plows into your car from behind, knocking you into the bus. Turns out the kid driving the full-sized crew cab pickup truck that hit you was texting, and never even hit his brakes. You're having a hard time remembering exactly what happened. You remember a flash of light and your head being slammed backwards over the top of your headrest. You vaguely recall that your head rocketed forward as you hit the bus, almost hitting the windshield. You step out of your vehicle to take a look at the situation. There is no blood and in fact, you don't even have a bruise to show from the incident. However, by the time the State Troopers arrive to access the accident, you not only have a neck pain unlike anything you have ever felt before, you have a banging headache as well. You're having trouble putting the pieces in order for them. They ask if you need an ambulance, but you do not want to go to the Emergency Room. But a few weeks later, you're still having trouble with your memory. Work is not going well because on top of the pain and exhaustion, everything seems fuzzy, foggy, and hazy. Who would have thought that whiplash could cause these sorts of symptoms, particularly without any obvious injuries?
Whiplash Injuries are particularly dangerous because they are a common cause of MTBI (Mild Traumatic Brain Injury). MTBI results from the brain bouncing off the inside of the skull during the hyperextension / hyperflexion of the neck. As you can imagine, this damages / destroys nerve cells. Depending on which part of the brain is injured, a person might have problems in some of the following areas:
- Walking / Moving
- Balance
- Coordination
- Strength / Endurance
- Your Ability to Communicate
- Your Ability to Understand
- Your Ability to Think
- Memory
- Strange or Unexplainable Pain Patterns or Symptoms
- Altered Psychological Profiles
FACTORS THAT WORSEN THE WHIPLASH INJURY:
WHAT CAN MAKE A WHIPLASH INJURY WORSE?
FACTORS THAT POTENTIALLYINCREASE WHIPLASH SEVERITY
|
FACTORS THAT POTENTIALLYDECREASE WHIPLASH SEVERITY
|
THE RELATIONSHIP BETWEEN SEVERITY OF INJURY AND THE AMOUNT OF AUTOMOBILE DAMAGE = NOTHING!!!

NEWTON'S LAWS OF MOTION:
In Principia, Newton laid out his three Laws of Motion. These laws are able to explain whiplash and the subsequent injury that follows better than anything else we have seen so far. For understanding whiplash injuries and their relationship to vehicle damage, Newton's first law is the most important; The Law of Inertia.
Newton's First Law: Objects at rest remain at rest unless they are acted on by an outside force. Likewise, objects in motion, stay in motion unless they are acted on by an outside force. Remember this - whiplash injuries occur because different parts of your body can and will have different inertias, sometimes very different inertias.
When your vehicle was struck from behind, it shot forward. When you were hit, there was a huge instantaneous change in momentum. In a fraction of a second, your vehicle was accelerated from zero to over 50 mph.
Let's look at this event in frame-by-frame fashion.
As your vehicle shot forward, so did your torso that was sitting in the seat. Here is the precise point where whiplash occurs. As your body was accelerated forward, your head (at least in the initial milliseconds) did not move. The head is much smaller (and lighter) than your torso, and attached by a thin column of muscles, tissues, and tiny vertebrate we call the neck or Cervical Spine. Because of the weight difference between the head and the body, as well as the fact that the connector between them (the neck) is stretchy and relatively thin; the head has a completely different inertia than the body. This was magnified by the fact that the seat back kept your torso from moving very far backwards, but did nothing to stop your neck, and unfortunately, your head restraint was not adjusted to the proper height. In other words, your body was essentially driven out from under your head, then a fraction of a second later, your head not only caught up with your body, it actually accelerated to a greater velocity than your body, and overshot it as your head slammed forward.
Let's review: As the vehicle, the seat, and your body rocketed forward with the explosive energy and momentum shift from the impact, your head remained stationary for a split second. Your body was essentially driven out from under your head, making it appear that your head slammed backwards. As your head's momentum began catch up to that of your body, the tissues in your neck began to stretch and deform. Unfortunately, when the force of the accident is greater than the forces holding your tissues together, these tissues begin to tear, at least on a MICROSCOPIC BASIS (remember, most of the time this tearing will not show up on an MRI). The result was a whiplash injury, an inertial injury to the SPINAL LIGAMENTS, SPINAL DISCS, FASCIA, TENDONS, and other soft tissues of the neck and upper back. In fact, there are studies showing that even though they are too small to be effectively imaged with current MRI technology, there are often (usually) microscopic fractures of the FACET JOINTS present with intense whiplash injuries. Frequently, there is also sub-clinical brain injury as well.
Interestingly enough, one of the things that make muscles contract with greater intensity is to maximally stretch them. When the neck is stretched to such a great degree, it's muscles contract to an equally intense degree. When coupled with the acceleration and subsequent deceleration of the vehicle, this causes the neck to slam forward causing still more tissue tearing in the neck and upper back. And the most important thing to grasp is that your neck and head never hit anything throughout the entire process. The injury to the neck itself (which happened in a matter of milliseconds) occurred because of a huge momentary shift in momentum, energy, and inertia between your body and your head, just like what you see in "Shaken Baby Syndrome".
Following an accident you have several spinal x-rays and a CT of your neck in the Emergency room. Everything is negative. The ER doctor comes in, examines you, and has you move a bit. He then you know "everything checked out fine, you may be sore so get the prescriptions filled to help you through any pain, and call your doctor in the morning. You'll be just fine."
But that's just it. You saw your doctor, and as the weeks go by, you're not fine. Far from it. You are in pain, and it's getting worse. But you have nothing to show for it, no borken bones, no bruises, cuts or scratches. There is nothing that would alert anyone (let alone a doctor who is not up on the most current research) that you are in pain, and it's getting worse. What's going on here? You want answers!
In 1964, the prestigious medical journal, American Journal of Orthopedics revealed a still well-concealed fact, that there is no relationship between the damage done to the vehicle and the amount of injury to the vehicle's occupants. Since that time, the medical and scientific communities have proved this fact over and over again via research. It is a fact that we have heard verified over and over again by the Law Enforcement Officers and Paramedics that we adjust on a regular basis. Although most of the time, Insurance Companies and the Attorneys that represent them would have you believe just the opposite (there was not enough vehicle damage to have an injury), it's just not true.
Decades worth of scientific studies tell us that the severity of the vehicle damage cannot predict:
- If patients will suffer whiplash injuries.
- How severe those injuries might be.
- How long it will take to effectively treat / heal the injury or whether they will ever really heal at all.
- Whether or not the injured party will end up with Chronic Pain and / or Arthritis as a direct result of the accident.
So, it stands to reason that harder impacts and greater amounts of vehicle damage lead to greater amounts of bodily injury. Not only is this not true, but most of the medical research on whiplash injuries today are being done on the effects of low speed impacts (those under 15 mph). Here are a few of the Scientific / Medical / Legal profession's journals saying that there is NO RELATIONSHIP between the amount of vehicular damage and the amount of injury to the vehicle's occupants.
- The Spine, 1982
- Orthopedic Clinics of North America,
- Society of Automotive Engineers, 1990
- Injury,
- Trial Talk,
- Injury,
- American Journal of Pain Management, 1994
- Society of Automotive Engineers,
- Society of Automotive Engineers,
- Archives of Physical Medicine and Rehabilitation,
- Journal Of Whiplash & Related Disorders,
- Spine,
- Journal of Neurology, Neurosurgery, and Psychiatry,
- Spine,
- Whiplash Injuries,
WHAT DOES THE SCIENTIFIC / MEDICAL / LEGAL LITERATURE SAY ABOUT ARTHRITIS AFTER A MOTOR VEHICLE ACCIDENT?
- Thus, it appeared that the injury had started the slow process of disc degeneration." The Cervical Spine Research Society, 1989
- The Cervical Spine Research Society, 1989
- The Journal of Orthopedic Medicine, 1997
- British Journal of Bone and Joint Surgery, 1983; The American Academy of Orthopedic Surgeons, 1987; Orthopedic Clinics of North America, 1988; Spine, 1994; British Journal of Bone and Joint Surgery, 1996
- European Spine Journal, 2004
WHIPLASH ASSOCIATED DISORDERS ARE DIFFICULT TO DIAGNOSE VIA ADVANCED IMAGING TECHNIQUES:
So just how should a problem like this be addressed? The key to a functional recovery is controlled motion. CHIROPRACTIC ADJUSTMENTS, specific stretches, and strengthening exercises are the number one way to accomplish this! Because FASCIAL ADHESIONS are usually part of the whiplash equation, you will probably need to undergo some form of Tissue Remodeling as well. Restoring movement, function, and strength (both to individual joints or vertebrate, and to the spine or limb as a whole) is the only proven method that is effective in truly reducing the symptoms of whiplash. Contrary to popular belief, using drugs to simply cover symptoms, is never a good option.
If the only treatment you receive for your whiplash injury is palliative (meaning covering symptoms with drugs, without addressing the underlying cause of those symptoms), then any relief achieved is temporary, and the end product of this process will likely be dysfunction, degeneration, and chronic pain!
MY DOCTOR SAYS HE CAN'T FIND ANYTHING WRONG WITH ME, AND THAT THE PAIN IS "ALL IN MY HEAD". WHAT DO I DO?
|
|
HYPERFLEXION / HYPEREXTENSION
OF THE CERVICAL SPINE:
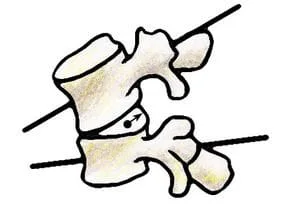
Photo by Joseph RENGER
|
With Hyperflexion, the spine goes forward, which drives the Nucleus of the disc to the back. This is why HERNIATED DISCS are a frequent result of Whiplash Injuries. In Hyperextension, the spine is slammed backward. Although this rarely if ever results in frontal Disc Herniations, it jams the facets (the two little joints to the rear and on either side of the disc). This can lead to a degenerative condition called FACET SYNDROME.
|

Photo by Joseph RENGER
|

SOFT TISSUE INJURIES
HOW LONG DO THEY TAKE TO HEAL?

THE PHASES OF TISSUE REPAIR AND HEALING:
- STAGE I (Inflammatory Phase): This phase lasts from 12-72 hours, and is characterized by a release of inflammatory chemicals by injured cells. When cells are injured and die, they rupture and release their contents into the extra cellular fluid / Inflammation. These “Inflammatory Chemicals” that are released from ruptured cells are a necessary and vital component of the healing process. However, in excessive amounts, they can cause a great deal of pain. They also promote excessive microscopic scarring. Be aware that if you visit your doctor for a soft tissue injury, you will be given anti-inflammatory medications. These have serious side-effects on the heart, liver, kidneys, etc. The fact that this class of drug has been scientifically proven to cause injured connective tissues to heal significantly weaker and with less elasticity than they otherwise would. Nowhere is this more true that CORTICOSTEROIDS. Do a quick search of the Medico-Scientific Literature on Corticosteroids and soft tissue injuries. You will see over and over again that they are detrimental to the healing process and should play no part in the treatment of these injuries.
- STAGE II (Passive Congestion): This phase begins by the 2nd to 4th day, we begin to see swelling (sometimes we do not see it, because it is not on the body’s surface). Remember; “inflammation” is not synonymous with swelling. Inflammatory Chemicals released by dying cells attract the fluid that causes swelling. This is why using cold therapy / ice to control both inflammation and swelling is such an important part of the healing process, particularly in its earliest stages. However, the best method for moving out this "Congestive Swelling" is through controlled motion if possible. Your medical doctor may tell you to use heat during these initial two phases of soft tissue healing; don't do it. Use ICE to control the inflammation!
- STAGE III (Regeneration & Repair Phase): The Repair Phase is where new collagen fibers are made by fibroblasts. The body then uses these collagen fibers as a sort of soft tissue “patch”. In the body, this collagen patch / scar tissue tends to be different than the tissue around it in a number of ways. Scar Tissue is weaker, less elastic, MUCH MORE PAIN SENSITIVE, has SEVERLY DIMINISHED PROPRIOCEPTIVE ABILITIES, etc). Be aware that the Repair Phase of tissue healing only lasts about 6 weeks, with the majority being completed in half that time. WARNING: This 3rd stage of healing is where many of the so-called “experts” want you to believe the process of Tissue Healing & Repair ends. Again; this phase is finished within a month of injury.
- STAGE IV (Maturation / Remodeling Phase): Not only is it the longest, but the Remodeling Phase is by far the most critical of thefour stages of Connective Tissue healing. Yet it is the phase that most often gets overlooked. The most current research shows that in case of serious Connective Tissue Injury, the Remodeling Phase can last up to two years; making the old “6-8 weeks” sound ridiculous. The Remodeling Phase is characterized by a “realignment” (remodeling) of the individual fibers that make up the injured tissue (the collagen “patch” that we call Scar Tissue). What is interesting is that each study that comes out on this topic, seems to be saying that this phase of healing lasts longer than what the study that came out before it said. This is a good thing. However, keep in mind that if you have not improved within 90 days after injury, standard forms of treatment become much less likely to help you. Phase IV can also be risky because although a person's pain may have dissipated, the injury itself has not completely healed and is vulnerable to re-injury.
As Controlled Loading / Tensile Loading is applied to the healing tissues via CHIROPRACTIC ADJUSTMENTS, TISSUE REMODELING, STRETCHING and strengthening exercises, PROPRIOCEPTIVE RE-EDUCATION, massage therapy, TRIGGER POINT THERAPY, PNF, etc; the individual tissue fibers move from a more random, tangled, and twisted wad of unorganized collagen fibrils; to a tissue that is much more organized, parallel, and orderly as far as its microscopic configuration is concerned. Again, this takes time. Although our Scar Tissue Remodeling Therapy can frequently bring immediate relief, it is obvious from the medical literature that there is a healing processes that cannot be bypassed. Because numerous Scientific Studies have proved Cold Laser Therapy to be effective in regenerating Collagen, we highly recommend it for our more seriously injured patients as well.
Everyone has heard the saying that is still used by doctors, "You would have been better off to break the bone than to tear the ligaments".. Knowing what we know about the healing of the Collagen-Based, Elastic Connective Tissues; this statement makes a lot of sense! Soft tissues heal much slower than other tissues (including bones). Do not let anyone try and convince you otherwise! This is why following the complete stretching and strengthening protocol that goes hand-in-hand with our “Tissue Remodeling” treatment, is the one and only way that it will work properly over the long haul. By the way, we have dealt extensively with the fact that whiplash injuries heal best with forms of therapy that employ controlled motion such as does chiropractic. Now I want to explore what the scientific literature says about using medications for whiplash injuries.
THE RELATIONSHIP OF INFLAMMATION TO PAIN AND SCAR TISSUE IN WHIPLASH INJURIES:
- Dolar (Pain)
- Calor (Heat)
- Rubor (Redness)
- Tumor (Swelling)---The chemicals we collectively call "inflammation" are not synonymous with swelling, but they can attract swelling.
- Functio Laesa (Loss of Function)
Although these chemicals can remain in a local area (you stub your toe, the toe gets red and inflamed), they can invade the blood stream and have a systemic (whole body) effect as well. But inflammation does not end there. These immune system chemicals that we refer to collectively as "inflammation" (prostaglandins, leukotrienes, thromboxanes, cytokines, chemokines, certain enzymes, kinnins, histamines, eicosanoids, substance P, and dozens of others) are being touted by the medical community as the primary cause of a whole host of physical ailments, when there are too many of them in the body. Some of the other problems that Inflammation is known to cause includes;
- Disc Injuries, Slipped Disc, Disc Herniation, and Disc Rupture
- Heart Disease and virtually all forms of Cardiovascular Problems
- Skin conditions including Eczema and Psoriasis
- Arthritis & Fibromyalgia
- Asthma
- ADD, ADHD, Depression, and various forms of Dementia
- Neurological Conditions
- Female Issues
- Cancer
- Inflammatory Bowel Disease / Leaky Gut Syndrome
- Diabetes, Insulin Resistance, Hypoglycemia, and other Blood Sugar Regulation Problems
- Obesity
Born in 1904, Dr. James Cyriax, a Cambridge-educated M.D. widely known as the "The Einstein of Physical Medicine" wrote his Magnum Opus, Orthopaedic Medicine, Diagnosis of Soft Tissue Lesions, in 1982 shortly before he passed away. Dr. Cyriax is still considered one of the brilliant pioneers of soft tissue research. One of Dr. Cyriax groundbreaking discoveries is that Scar Tissue / Fibrosis can and will generate an Inflammatory Response long after the Fourth stage of Healing Maturation & Remodeling is over. Pay attention to what Cyriax wrote over three decades ago.
|
|
"Fibrous tissues appears capable of maintaining an inflammation, originally traumatic, as the result of a habit continuing long after the cause has ceased to operate. It seems that the inflammatory reaction at the injured fibers continues, not merely during the period of healing, but for an indefinite period of time afterwards, maintained by the normal stresses to which such tissues are subject."
|
|
Why would what Dr. Cyriax refers to as "normal mechanical stresses" cause an "indefinite period" of inflammation? Scar Tissue and Fibrosis are so dramatically different from normal tissue. One of the most obvious ways that this can be seen is by looking at any good Pathology Textbook. Scar Tissue and Fibrosis is far weaker and much less elastic than normal Connective Tissue. What does this mean? Only that it is easily re-injured. This starts the whole vicious cycle over again. Injury ----> Inflammation ---> Pain ---> Fibrosis & Scar Tissue Formation ---> Re-injury ---> Repeat indefinitely. Just remember that the end result of this cycle is DEGENERATION of the affected bones and spinal discs.

SCAR TISSUE & FIBROSIS IS DIFFERENT FROM NORMAL TISSUE IN THREE MAIN WAYS:
SCAR TISSUE IS WEAKERRepaired soft tissues are weaker than the body's undamaged soft tissues. The diameter of the collagen fibers of scar tissue are smaller than those of normal tissue. Also, as you can see from the pictures above, the structure has been physically changed. This weakness leads to a viscous cycle of instability, re-injury, and degeneration.
|
SCAR TISSUE IS LESS ELASTICRepaired soft tissues are always less elastic and "stiffer" than the body's undamaged soft tissues. This has to do with the fact that the individual collagen fibers will never identically align themselves quite like the original uninjured soft tissue. This is all easy to see because range of motion testing on injured individuals will always show areas of decreased ranges of motion.
|
Repaired soft tissues have a strong tendency to be more pain-sensitive than their uninjured counterparts. In fact, for reasons that are not completely understood, Scar Tissue has the neurological capability of going into something called "super-sensitivity", and can end up 1,000 times more sensitive to pain than normal tissue.
|
MORE ON THE RELATIONSHIP BETWEEN INFLAMMATION, PAIN, AND FIBROSIS / SCAR TISSUE:
Chronic Inflammation of a whiplash injury leads to Scar Tissue Formation, and Scar Tissue Formation leads to even more pain. And like I mentioned earlier, the whole mess leads to Spinal Degeneration. How can you break free? Dr. Cyriax goes on to say in his book that immobilization of injured soft tissues is a bad thing, and mobilization of injured soft tissues is not only good, but necessary for proper healing to take place. But under the umbrella of America's medical drug culture, functional restoration frequently takes a back seat to different kinds of medicines. However, if you need something for the pain after a whiplash injury, there is no dishonor in doing something on a short-term basis. However, this is never the solution. It is masking symptoms to get you through a rough place. As long as you understand this, OK. However, there is one class of drugs that should play no part in the healing of your Whiplash Injury.
THE EFFECTS OF INFLAMMATION MEDICATIONS ON WHIPLASH INJURIES AND SOFT TISSUE INJURIES IN GENERAL:
- New England Journal of Medicine, 1994
- New England Journal of Medicine, 1997
- New England Journal of Medicine, 1999
- Spine, 2003 & Surgical Neurology, 2006
- Hypertension, 2005
- European Heart Journal, 2006
- Drug Safety, 2009
- Drug Safety, 2009
- Neurology, 2009
So, what is a person supposed to do? Despite decades of research saying that NSAID's are not "therapeutic" (actually helps you get better), but are instead, "palliative" (makes you feel better without any therapeutic benefits), the medical community continues to hand these and other dangerous drugs out almost like candy. Just remember that any pain relief achieved without addressing the underlying components of the Whiplash Injury, are temporary. And that's not all. When joints and tissues heal in RESTRICTED FASHION, they always end up with copious amounts of DEGENERATION. And the final kick in the teeth for those of you who have been on this MEDICAL MERRY-GO-ROUND is that much of this research is at least two decades old. As we have said for a very long time, much of the medical community is caught in a time warp. They are treating whiplash injuries using outdated models, often times very outdated models. Again we ask; what's a person to do? How about WHAT WE HAVE TO OFFER OUR PATIENTS here at Breidenbach Chiropractic?
CHIROPRACTIC BENEFITS FOR WHIPLASH PATIENTS WHO STRUGGLE WITH BACK AND NECK PAIN:
- American Journal of Anatomy, 1940
- Journal of the American Medical Association, 1958
- Textbook of Orthopedic Medicine, 1982 & Continuous Passive Motion, 1993
- Canadian Family Physician, 1985
- British Medical Journal, 1991
Lancet, 1991 - Injury, 1996
- Annals of Internal Medicine, 2002
- Spine, 2003
- Journal of Manipulative and Physiological Therapeutics, 2005
- DEGENERATIVE ARTHRITIS, 59% can eliminate their pain medications by taking omega-3 fatty acids found in fish oil (EPA & DHA). Surgical Neurology, 2006
- A Review of the Evidence for the American Pain Society and the American College of Physicians Clinical Practice Guideline”, only spinal manipulation was touted as effective for the treatment of both acute and chronic low back pain. Annals of Internal Medicine, 2007
- Chiropractic care is more effective than other modalities for treating low back and neck pain”. Do Chiropractic Services for the Treatment of Low Back and Neck Pain Improve the Value of Health Benefits Plans? An Evidence-Based Assessment of Incremental Impact on Population Health and Total Health Care Spending, 2009
LONG TERM PROGNOSIS FOR WHIPLASH PATIENTS;
- Journal of Bone and Joint Surgery published research in 1964 showing that of 145 patients involved in a study of whiplash injuries; as many as 83% of the injured patients continued to suffer from pain two years after the accident. If the symptoms resulting from an extension-acceleration injury of the neck are purely the result of litigation neurosis, it is difficult to explain why 45%of the patients should still have symptoms two years or more after settlement of their court action."
- Neuro-Orthopedics published a study was carried out on patients suffering with whiplash for well over a decade. Despite the length of time involved, nearly two thirds still struggled with moderate to severe pain symptoms due to their accident. "If symptoms were largely due to impending litigation it might be expected that symptoms would improve after settlement of the claim. Our results would seem to discount this theory, with the long-term outcome seeming to be determined before the settlement of compensation."
- Journal of Clinical Epidemiology showed that 40% of those suffering an accident-induced whiplash injury continued to suffer from neck and shoulder pain seven years post-accident.
- Injury, showed that over 20% of those injured in a whiplash injury struggled with Chronic Pain nearly 8 years post-injury. Furthermore, almost half of those in the study suffered from "Nuisance Pain" during the same time frame.
- British Journal of Bone and Joint Surgery showed 40% of the whiplash patients struggling with Chronic Pain over a decade after the fact. 40% of the remainder of the study's people dealt with "Nuisance Pain" during the same period. The fact that symptoms do not resolve even after a mean 10 years supports the conclusion that litigation does not prolong symptoms."
- British Journal of Bone and Joint Surgery reported that well over 40% of whiplash-injured patients struggled with Chronic Pain from the accident over a decade and a half after the fact. Almost 30% of the rest dealt with "Nuisance Pain" over the course of the study. "Symptoms did not improve after settlement of litigation, which is consistent with previous published studies".
- European Spine Journal published a nearly two decade long study on whiplash-injured patients in 2002. Well over half (55%) of those studied had pain seventeen years post-accident. One quarter of these dealt with daily neck pain, and almost one quarter had radiating arm pain on a daily basis. "It is not likely that the patients exposed to motor vehicle accidents would over-report or simulate their neck complaint at follow-up 17 years after the accident, as all compensation claims will have been settled."
- British Journal of Bone and Joint Surgery looked at whiplash-injured patients three decades after their initial injury. 15% of these patients struggled with daily pain severe enough to require treatment. Four out of ten of the remainder dealt with "Nuisance Pain" over the same time frame.
ATTORNEY'S, INSURANCE COMPANIES, FEES, & MED PAY:
WHERE DOES THIS ALL LEAD?
After their attorney reaches a settlement for their injured client, any treatment they were receiving typically ends. As you can see, the treatment frequently ends without ever effectively dealing with the underlying scar tissue and FASCIAL ADHESION that leaves so many people in Chronic Pain, long after they have settled their injury claim.
These individuals enter the miserable world of CHRONIC NECK / BACK PAIN and HEADACHES, and then wonder what they are going to do because their $3,000 settlement check is long gone. The patient is then left with a choice. They can climb back on the MEDICAL MERRY-GO-ROUND and continue to go round in circles. Tests, blood work, MRI’s, CT scans, drugs, drugs, and more drugs; and therapy — more of the same (expensive) stuff you went through before you settled your case, with more of the same unanswered/unresolved results. Or you can do something different.
If you have a Med Pay Policy tacked on to your auto insurance, we will file it for you. Med-Pay is a small injury policy that you can attach to your auto insurance policy for a very small amount of money. Because attorneys cannot touch your Med-Pay (yet), it is the one form of Automobile Insurance that we will sometimes accept assignment on.
MED-PAY AUTOMOBILE ACCIDENT / INJURY INSURANCE POLICIES:
Most people who add Med Pay to their auto insurance policy understand what it is there for. Med Pay is nothing more than a small health insurance policy that covers accident-related injuries that occur while in your automobile. Many people tend to add it because the cost of a Med-Pay policy is inexpensive.
Please know that no matter what your insurance agent or adjuster tells you, filing a Med Pay claim on your own automobile insurance policy will not make your insurance rates go up - EVEN IF THE ACCIDENT WAS THE OTHER PERSON’S FAULT ! This is exactly what Med Pay is for. A Med-Pay policy typically means little or no out of pocket expense for you.
PREVENTING WHIPLASH INJURIES OR LESSENING THEIR EFFECTS:
- DRIVE A SAFE VEHICLE: Make sure that the vehicle you drive is highly rated by the organizations that rank automobile safety.
- DRIVE SAFELY AND DEFENSIVELY: This is common sense and one of the major facts most of us learned prior to getting our drivers license. Things happen quickly, that you have no control over. However, driving your automobile in an unsafe manner definitely puts you at a higher risk for suffering a Whiplash Injury.
- WEAR YOUR SEAT BELTS: The simple truth of the matter is that seat belts will probably not lessen the "Whiplash" component of an Automobile Accident. In fact, by holding your body in place while your head flies around, they can potentially worsen a neck injury to the soft tissues. However, seat belts will help to keep you alive.
- MAKE SURE YOUR HEAD REST/RESTRAINT IS ADJUSTED PROPERLY: This is by far the most important thing you can do diminish your chances of Whiplash Injury should you end up in an MVA. The truth is, most of us refer to these things that stick out of the top of our seats as "Head Rests" instead of "Head Restraints", and actually have them adjusted improperly (all the way down). The purpose of these devices is not to "rest" your head because you are tired, it is to "restrain" your head from flying backwards during a rear-ender accident. The top of the Head Restraint should be level with the top of your head, and the gap between the two should not be more than about two inches. For the record; if you recline your seat more than 20 degrees, all bets are off. A serious rear-ender will cause you to curl up in your seat rendering the Head Restraint useless.
HELPFUL WHIPLASH LINKS:
- DR FRANK PAINTER'S WHIPLASH PAGE
- THE SPINE RESEARCH INSTITUTE OF SAN DIEGO
- CHIROPRACTIC IS THE ONLY "PROVEN" TREATMENT FOR WHIPLASH
- MULTIPLE STUDIES CONFIRM POSITIVE OUTCOMES OF CHIROPRACTIC CARE FOR WHIPLASH INJURIES
- THE WORLD'S TOP FORENSIC MOTOR VEHICLE ACCIDENT RECONSTRUCTION EXPERT
- SETTLE YOUR OWN INJURY CLAIM
